Tesamorelin for visceral fat: what the research actually shows
Most fat loss conversations focus on the fat you can see and pinch. But the fat that actually matters for your metabolic health is the kind you can't see at all, and it's far harder to shift through diet and exercise alone.
Visceral fat, the fat wrapped around your organs, drives insulin resistance, raises cardiovascular risk, and secretes inflammatory compounds that quietly damage your health over time. There is one peptide that has been specifically studied and FDA-approved to target it. It's called tesamorelin, and the clinical data behind it is genuinely compelling. Here's what the research shows, who it's most relevant for, and the one side effect that gives me pause as someone who specialises in insulin resistance.
The two types of fat, and why only one is dangerous
Not all body fat is created equal, and this distinction matters more than most people realise.
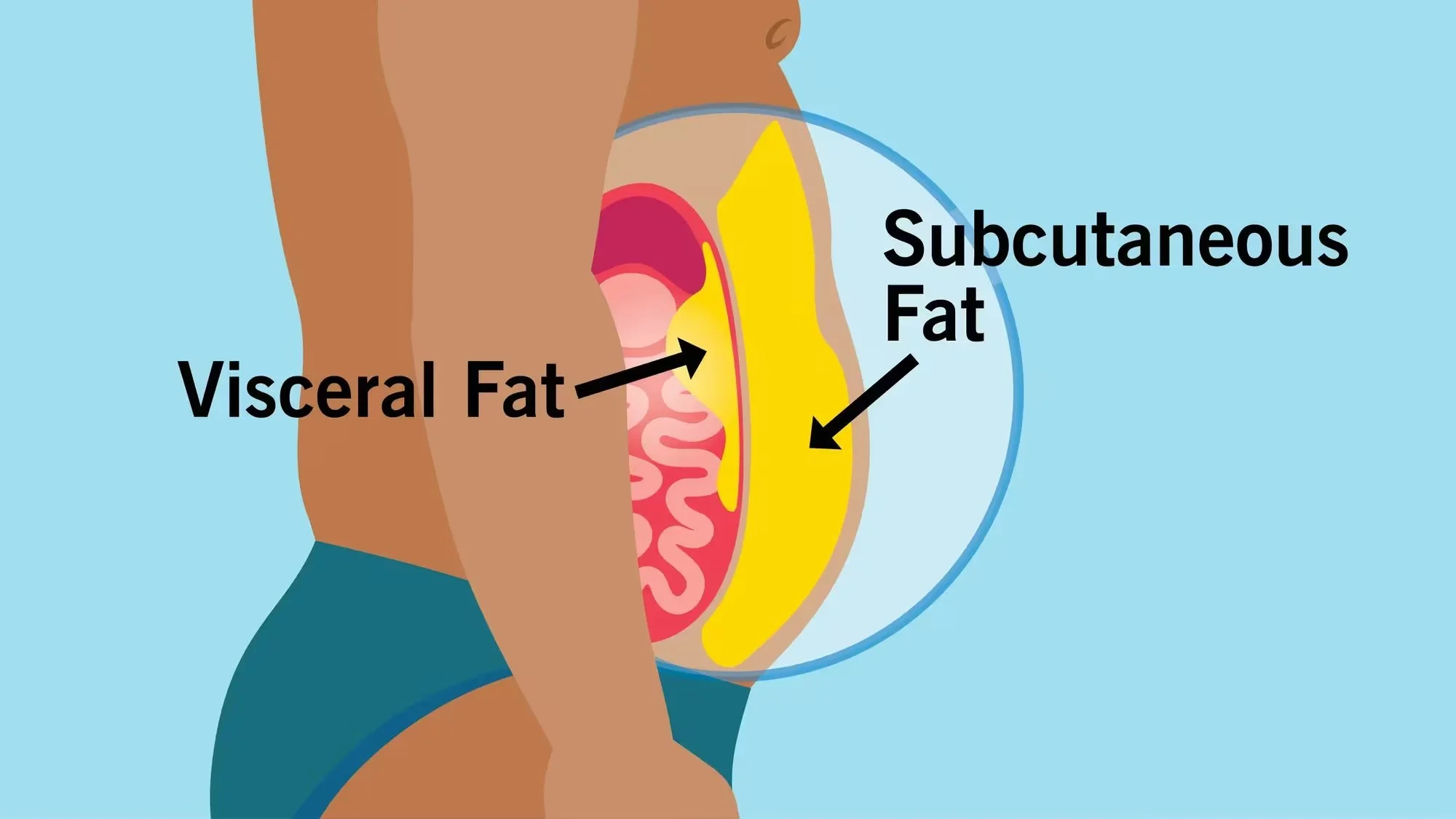
Subcutaneous fat is the fat just under your skin, the kind you can pinch. It's essentially your body's stored energy reserve. Not ideal in excess, but not acutely dangerous either.
Visceral fat is different. It sits deep inside the abdominal cavity, wrapped around your liver, pancreas, and intestines. You can carry a significant amount of it without looking obviously overweight. What makes it dangerous is that it's metabolically active. It secretes inflammatory compounds, drives insulin resistance, and is strongly linked to cardiovascular disease.
The common claim that you can't spot-reduce fat applies to subcutaneous fat. Visceral fat responds to different inputs entirely, and that's what makes tesamorelin worth understanding.
Why visceral fat is so hard to lose
Visceral fat accumulation isn't just about calories. Three major drivers are often overlooked.
Chronic stress and cortisol. Visceral fat is highly sensitive to cortisol. This is why people who eat well and exercise can still carry significant visceral fat if their stress and sleep aren't managed. Chronic cardio without adequate recovery can actually contribute to visceral fat accumulation rather than reduce it.
Insulin resistance. The relationship goes both ways. Visceral fat makes you more insulin resistant, and insulin resistance leads to more visceral fat. Breaking this cycle requires more than calorie restriction.
Declining growth hormone. This is the factor most people aren't aware of. Growth hormone plays a direct role in fat metabolism, specifically visceral fat. It starts declining in your late 20s and continues steadily, which is why visceral fat tends to accumulate through your 30s and 40s even when diet and lifestyle haven't significantly changed. It's not entirely your fault. It's partially hormonal.
This last mechanism is exactly what tesamorelin works on.
What tesamorelin is and how it works
Tesamorelin is a synthetic analog of growth hormone releasing hormone (GHRH). Rather than injecting growth hormone directly, it stimulates your body to produce more of its own.
This distinction matters. Injecting growth hormone directly can suppress your body's natural production over time. Tesamorelin works with your existing system rather than replacing it, which gives it a more favourable safety profile than direct growth hormone administration.
The increased growth hormone then drives an increase in IGF-1 (insulin-like growth factor 1), the downstream signal that carries out many of growth hormone's effects in the body, including the breakdown of visceral fat.
[IMAGE: simple graphic showing the GHRH, growth hormone, IGF-1, fat metabolism pathway]
Tesamorelin was originally developed and received FDA approval for the reduction of abdominal fat in people with HIV, where treatment side effects caused abnormal fat distribution. This is the clinical context in which the most rigorous data was collected.
What the clinical trials actually showed
The pivotal trials for tesamorelin were published in the New England Journal of Medicine, some of the most rigorous data available on any peptide in this space.
Participants saw a reduction in visceral fat of approximately 15 to 18% over 26 weeks. Critically, these results were measured using DEXA and CT scans, not just waist circumference, meaning actual visceral fat volume was tracked rather than a proxy measure. Triglycerides also decreased significantly in the treatment group, which aligns with the mechanism.
One important caveat: many participants regained visceral fat after stopping the peptide. This pattern is consistent with what we see across weight loss peptides more broadly. The window while you're on the peptide is an opportunity to build the habits, sleep, nutrition, stress management, resistance training, that will sustain results when you stop. Peptides are a tool, not a cure.
Side effects worth knowing about
The clinical data gives us a reasonably clear picture of what to expect.
Common side effects include injection site reactions such as redness, itching, and swelling. These are typical of many peptides and generally not harmful.
More notable are fluid retention and joint pain, though for most people these resolve within a few weeks.
The side effect I'm most cautious about as someone who specialises in insulin resistance is the potential impact on insulin sensitivity. Tesamorelin increases growth hormone and IGF-1, and elevated growth hormone can reduce insulin sensitivity in some people. The trial data showed this effect was moderate for most participants, but it's worth flagging because insulin resistance is one of the primary drivers of visceral fat in the first place. Improving insulin sensitivity is part of addressing the root cause, so this is a dynamic worth monitoring closely.
As with most peptides outside of their approved indications, tesamorelin is research use only in most countries. That landscape is changing as more research emerges, and it's worth being informed for when it does.
Who is most likely to benefit
Based on the mechanisms and the research, here's how I think about who tesamorelin is most relevant for.
Best candidates: People in their 40s and above carrying significant visceral fat, particularly the kind associated with declining growth hormone. A pronounced midsection with otherwise relatively healthy lifestyle habits is a common profile here.
Less relevant: People under 40 where growth hormone is still relatively robust. For this group, the potential cons likely outweigh the benefits.
Not a substitute for foundations: Diet, sleep, stress management, and resistance training should always be the first line of approach. Tesamorelin may be worth considering as an accelerant once those foundations are in place, not instead of them.
Key takeaways
Visceral fat is metabolically dangerous in a way subcutaneous fat is not, and requires a different approach to shift
Declining growth hormone from your late 20s onwards is a major but underappreciated driver of visceral fat accumulation
Tesamorelin stimulates your body's own growth hormone production rather than replacing it, which gives it a more favourable safety profile than direct growth hormone
Clinical trials showed 15 to 18% reduction in visceral fat over 26 weeks, measured by DEXA and CT scan
The potential impact on insulin sensitivity is worth monitoring, particularly if insulin resistance is already a concern
Results don't last without sustainable habits built during the peptide window
Currently research use only outside of its approved HIV-related indication in most countries
FAQ
What is tesamorelin used for? It was originally FDA-approved to reduce excess abdominal fat in people with HIV-associated lipodystrophy. It's now being studied more broadly for its effects on visceral fat reduction related to age-related growth hormone decline.
How is tesamorelin different from growth hormone injections? Rather than introducing growth hormone directly, tesamorelin stimulates your body to produce more of its own via the GHRH pathway. This works with your body's natural systems rather than bypassing them, which generally means a better safety profile and less risk of suppressing your own production.
How much visceral fat can tesamorelin reduce? Clinical trials published in the New England Journal of Medicine showed approximately 15 to 18% reduction in visceral fat volume over 26 weeks, measured by DEXA and CT scans.
Is tesamorelin safe for people with insulin resistance? This requires careful consideration. Elevated growth hormone can reduce insulin sensitivity in some people, and since insulin resistance is a key driver of visceral fat, it's an important dynamic to monitor. Anyone with existing insulin resistance should discuss this closely with a healthcare professional.
Can you get tesamorelin from a doctor? Outside of its approved use for HIV-related fat redistribution, tesamorelin is research use only in most countries and is not available via standard prescription. The regulatory landscape around peptides is evolving, and wider availability may follow as more research accumulates.
Conclusion
The research behind tesamorelin is some of the most rigorous data available on any peptide specifically targeting visceral fat, and a 15 to 18% reduction in visceral fat volume is a meaningful result. For people in their 40s and beyond carrying significant visceral fat, it's worth understanding.
That said, the potential impact on insulin sensitivity means I'm watching this one carefully. Watch the full YouTube video for a deeper breakdown, including how tesamorelin compares to retatrutide and why the mechanism difference matters. And if there's another peptide you'd like me to cover, drop it in the comments.